Volume 1, Issue 2
Article Type: Research Article
Advancements in safe fall landing strategies: An updated systematic review
Shannon Dudash, PT, DPT1*; Edmund Ickert, PT, DPT, PhD1; Weiqing Ge, PT, DPT, PhD1; Hannah Crites2; Colleen Duchon3
1Assistant Professor, Department of Graduate Studies in Health and Rehabilitation Sciences, Youngstown State University, USA.
2Assistant Director, Student Development, YSU Sokolov Honors College, Youngstown State University, USA.
3Reference Librarian, Northeast Ohio Medical University, USA.
*Corresponding author: Shannon Dudash
Assistant Professor, Department of Graduate Studies in
Health and Rehabilitation Sciences, Youngstown State University, One Tressel Way, Youngstown, OH 44555, USA.
Tel: (330) 941-2407, Fax: (330) 941-1898;Email ID: Sstarr@ysu.edu
Received: Jul 15, 2025
Accepted: Aug 05, 2025
Published Online: Aug 12, 2025
Journal: Annals of Gerontology and Geriatrics
Copyright: Dudash S et al. © All rights are reserved
Citation: Dudash S, Ickert E, Ge W, Crites H, Duchon C. Advancements in safe fall landing strategies: An updated systematic review. Ann Gerontol Geriatr Res. 2025; 1(2): 1015.
Abstract
Background: Falls among older adults are a leading cause of injury, morbidity, and mortality. While traditional fall prevention programs emphasize balance and strength, emerging evidence highlights the potential of teaching safe landing strategies to reduce injury severity during unavoidable falls.
Objective: To conduct an updated systematic review evaluating recent advancements in safe fall landing techniques, their biomechanical effects, and the feasibility of implementing these strategies to reduce impact severity and injury risk.
Methods: A systematic search of PubMed, Web of Science, CINAHL, and Cochrane Library databases was conducted for studies published between January 2016 and July 2023. Eligible studies included human participants and reported kinetic or kinematic impact severity outcomes related to fall landing strategies. Data were extracted on study design, intervention type, participant characteristics, and biomechanical outcomes. Risk of bias was assessed using the Cochrane RoB 2.0 tool for randomized trials and ROBINS-I for non-randomized studies.
Results: Six studies met inclusion criteria, including randomized controlled trials and biomechanical analyses of fall simulations in older adults, young adults, and children. Findings demonstrated that techniques such as tuck-androll maneuvers and backward fall strategies significantly reduced head and hip impact forces. Training programs effectively improved motor responses and reduced fall impact severity, with skill retention observed in both older adults and pediatric participants. However, substantial heterogeneity in study designs, populations, and outcome measures precluded meta-analysis.
Conclusions: Safe landing strategies, including tuck-androll techniques and progressive fall training programs, may reduce impact severity and may be feasibly implemented in older adults. Current evidence is limited by small sample sizes and lack of long-term data. Future research should prioritize larger trials, standardized outcome measures, and assessment of real-world injury prevention. Integrating fall landing training into comprehensive fall prevention efforts may enhance safety, particularly for at-risk older adults.
Keywords:Fall or falls; Fall prevention; Fall landing strategies.
Introduction
Falls are a major public health concern among older adults, often resulting in severe injuries, reduced mobility, and increased mortality [1-3]. Each year, one in four older adults experiences a fall, contributing to over 3 million emergency room visits and 38,000 deaths [1,2]. The financial burden of fall-related injuries in the United States is projected to exceed $101 billion by 2030 [1,2]. Despite the availability of numerous evidence-based fall prevention strategies, the incidence of falls, associated injuries, and healthcare costs continue to rise [1]. As a result, an alternative approach looks at understanding and implementing safe landing strategies as a potential approach to reducing these adverse outcomes.
There have been various research studies that have identified potential landing strategies as part of a fall prevention program. In their systematic review and meta-analysis, Moon and Sosnoff identified seven effective landing strategies—squatting, elbow flexion, forward rotation, martial arts rolling, martial arts slapping, muscle relaxation, and stepping—that significantly reduce impact forces during falls [4]. Building on these findings, recent studies have further explored the benefits of fall landing techniques for older adults [5-9]. One such study examined the Judo4Balance program, which teaches and reinforces safe falling strategies, demonstrating that older adults can successfully learn and develop proficiency in these techniques [7]. Similarly, research on Ditangquan exercises, a form of traditional Chinese martial arts, found that incorporating safe landing strategies not only improves functional mobility in older adults but also reduces fall frequency and injury severity while enhancing their confidence in fall prevention [9].
Although research on the use of fall landing strategies to improve physical measures, enhance fall efficacy, and reduce falls has emerged since the 2017 systematic review, it remains limited. Before conducting further trials on safe landing techniques, it is essential to assess the latest evidence on reducing impact forces and implementing these strategies effectively. This updated systematic review aims to synthesize recent advancements in safe fall landing techniques, evaluate their effectiveness, and provide comprehensive insights to guide clinical practice and public health interventions.
Methods
This review is reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Statement for systematic reviews and meta-analyses [10]. The protocol was registered with the International Prospective Register of Systematic Reviews (registration number CRD42023441977).
Search strategy
A comprehensive literature search was conducted in collaboration with a research librarian. Drawing from the original systematic review, the librarian refined the search terms and performed the initial database search. The search was conducted for studies published from January 2016 to July 2023 using the following electronic databases: PubMed, Web of Science, Cumulative Index to Nursing and Allied Health Literature (CINAHL), and the Cochrane Library. A keyword search was performed using all possible combinations (including wildcard characters) from four thematic groups:(1) fall OR falls OR “sideways falls” OR “lateral falls” OR “forward falls” OR “backward falls”; (2) technique* OR training OR strategy* OR protective OR response* OR reflex; (3) “femoral fracture” OR “hip fracture” OR “hip impact” OR “wrist fracture” OR osteoporosis OR “bone fracture”; and (4) biomechanic* OR kinematic* OR kinetic* OR EMG OR “muscle activation” OR velocity OR force.
Study selection
All database search results were merged and uploaded to Microsoft Excel (Microsoft Corporation) with duplicate records removed. The remaining papers were first screened on the title and subsequently on the abstract, performed by two authors independently (E.I. and S.D.). The remaining papers were then examined at the full-text level independently by the same two authors. Any disagreements for inclusion were resolved between the reviewers throughout each stage by discussion and consensus. If resolution did not occur, a third author (W.G.) was available to resolve disputes.
For this updated systematic review, the same study selection criteria were applied to ensure consistency in evaluating the effectiveness of fall landing strategies. Studies were included if they met all of the following criteria: (1) study design: randomized controlled trial, cohort study, pre-post study, or cross sectional study; (2) subjects: human participants; (3) main outcome: kinetic or kinematic impact severity measurements, including impact velocity, impact force, fall duration, and impact angle; and (4) language: English.
Studies were excluded if they met one or more of the following criteria: (1) relied solely on computer simulations; (2) employed a nonexperimental design (e.g., questionnaire-based study); (3) did not include kinetic or kinematic impact severity measurements; (4) involved fall simulations without ground impact; (5) lacked comparative analysis of different falling strategies; (6) were published in a language other than English; (7) were review articles or case studies; or (8) were not peer-reviewed (e.g., dissertations, conference proceedings).
Data extraction
A standardized data extraction form, consistent with the original review, was employed to gather methodological and outcome variables from each included study. These variables included: author(s), year of publication, study design, type of protective landing strategy, comparative normal landing strategy, fall simulation details (e.g., self-initiated vs. unexpected falls, standing vs. kneeling positions, fall direction, and instructions provided), impacted body region, sample size, participant characteristics (e.g., sex, age, height, weight), and measures of impact severity (e.g., impact velocity, kinetic energy, force, duration, and angle).
Quality assessment
Risk of bias was independently assessed by two reviewers (W.G. and H.C.) for all included studies. For randomized controlled trials, the Cochrane Risk of Bias 2 (RoB 2) tool was utilized, following the guidance of the Cochrane Handbook for Systematic Reviews of Interventions [11]. This tool evaluates five domains of potential bias: the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each domain was assigned a judgment of “low risk,” “some concerns,” or “high risk,” and an overall risk of bias was determined for each study.
For non-randomized studies, the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool was used [12]. This tool assesses bias related to confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of the reported result. Each domain was rated as having “low,” “moderate,” “serious,” or “critical” risk of bias, and an overall risk of bias was assigned accordingly.
Any disagreements between reviewers were resolved through discussion. If consensus could not be reached, a third reviewer (S.D.) was consulted to determine the final judgment.
Data synthesis
Data synthesis focused on comparing the effects of various fall landing strategies or educational interventions on outcomes related to fall impact severity. Studies included in the review assessed landing strategies such as backward fall techniques, tuck-and-roll maneuvers, and safe landing training programs among populations ranging from older adults to children. Due to heterogeneity in study designs, populations, and outcome measures, a meta-analysis was not feasible. Therefore, a narrative synthesis of findings was conducted.
Key outcomes extracted for synthesis included measures of impact severity such as peak acceleration, force upon impact, fall duration, and impact velocity. Where available, comparisons were made between intervention groups trained in a specific fall technique (e.g., backward fall, tuck-and-roll) and control groups that either received no fall training or practiced a standard or natural fall response. In randomized controlled trials, the intervention arms that included safe fall education were directly compared with those receiving usual activity or balance training without targeted fall strategies.
When multiple experimental conditions were reported in a single study (e.g., different fall directions or fall initiation methods), results were described separately to preserve contextual clarity. Due to variation in fall simulation protocols (e.g., kneeling vs. standing, self-initiated vs. externally perturbed falls), findings were grouped descriptively according to fall direction, population age, and training intervention type.
All statistical analyses and descriptive summaries were performed using Review Manager Web (Cochrane Collaboration) and SPSS version 28.0 (IBM Corp., Armonk, NY, USA). Inter-rater reliability during study selection, risk of bias assessment, and certainty of evidence grading was calculated using Cohen’s weighted kappa (κ). Kappa values were interpreted as follows: ≤0 = no agreement; 0.01–0.20 = slight agreement; 0.21–0.40 = fair agreement; 0.41–0.60 = moderate agreement; 0.61–0.80 = substantial agreement; and 0.81–1.00 = almost perfect agreement [13].
Results
Study selection
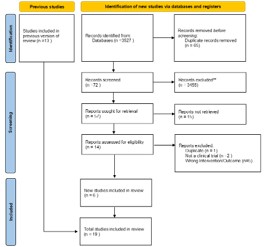
A total of six studies met the inclusion criteria and were included in this systematic review [5,7,14-17]. These studies examined the biomechanical and educational impacts of fall landing strategies in diverse populations, including older adults and children. Figure 1 illustrates the PRISMA flow diagram detailing the selection process. Inter-rater reliability was substantial for title screen inclusion (κ=0.744), abstract screen inclusion (κ=0.801), and almost perfect for full-text review inclusion (κ=0.857).
Study characteristics
The included studies were published between 2017 and 2023 and varied in design, including Randomized Controlled Trials (RCTs), quasi-experimental studies, and biomechanical analyses of fall simulations. Sample sizes ranged from 12 to 138 participants. Populations studied included community-dwelling older adults, children, and young adults. A detailed summary of study characteristics is provided in Table 1.
Methodological quality
Quality appraisal was conducted using the Cochrane Risk of Bias 2.0 tool for RCTs and the ROBINS-I tool for non-randomized studies. Four studies demonstrated overall low risk of bias, with common concerns related to outcome measurement and selection bias in observational designs [14-17]. The two RCTs were found to have some concern [5,7]. Detailed risk of bias assessments are provided in Table 2.
Fall landing strategy interventions and outcomes
Each study assessed different fall landing strategies aimed at reducing biomechanical impact during falls. The following key findings were observed:
Head impact reduction: Three studies investigated head impact in backward and sideways falls [5,14,15]. Using the sagittal acceleration of the head as a metric, backward fall techniques (e.g., chin-tuck and arm positioning) demonstrated significantly reduced head acceleration. Age-related differences were also observed, with older adults experiencing greater head acceleration during sideways falls compared to younger participants, indicating diminished protective response with aging [14].
Hip impact and fall characteristics: Fall characteristics such as direction, fall height, and velocity influenced hip impact severity [17]. Falls from a standing position onto the side led to greater kinetic energy and impact force compared to more controlled falls [5,17].
Learning and retention of fall techniques: Three studies assessed the ability of older adults and children to learn and retain safe fall strategies [5,7,16]. Programs teaching the “tuckand-roll” and backward fall techniques resulted in significantly reduced impact forces and improved motor responses during induced falls [5]. Improvements were retained over short follow-up periods, indicating feasibility of such training in both clinical and community settings.
Training approaches: High-challenge exercises and progressive safe-landing drills were effective in enhancing performance of protective responses. Notably, participants in structured training programs showed improved motor patterns and reduced fall impact metrics compared to untrained controls [5,7,15,16].
Table 1: Study characteristics.
| First author/year | Fall direction | Subjects | Participant characteristics | Design | Intervention/landing strategy | Key outcomes |
|---|---|---|---|---|---|---|
| Moon et al 2019 | Sideways | 14 (7= control; 7= intervention) | Adults 55-75 yo | RCT | 2 training sessions for 30 and 60 min each; Tuck and roll fall landing training | Hip impact force, hip impact velocity, head acceleration |
| Arkkukangas et al 2022 | Forward, Sideways, Backwards | 79 (42= control; 37= intervention) | Adults >65yo | RCT | 12-week; Judo4Balance | Observation of Falling techniques forward, backward, sideways; Mini- BESTest; FES-S; Activity level; EuroQoL- 5D-3L |
| Wood et al 2019 | Sideways | 25 | 15 Adults (21.2±2.7) 10 Adults (61.9±4.3) |
Observational | No Intervention | Head impact and head acceleration |
| Lim and Choi 2020 | Forwards, Sideways, Backwards | 20 | Adults 19-27yo | Observational | No Intervention | Hip impact force with different knee positions |
| Del Castillo- Andres et al 2018 | Backwards | 122 | Children 10-12yo | Quasi- Experimental | 6 week; education on falls and training on Safe Fall program | Information Scale on Safe Ways of Falling ad-hoc observation scale (measures 5 physical reactions during backwards fall) |
| Mroczkowski 2022 | Backwards | 41 | Adults 19-26 yo (19 martial arts trained; 22 handball trained) | Observational | No intervention; compared 2 groups of students who were trained in martial arts and handball | Sagittal linear acceleration of head |
Key: RCT: Randomized Control Trial
Table 2: Risk of bias assessment for included studies.
| Study | Risk of bias tool | Randomization / confounding | Deviations from intended intervention | Missing outcome data | Outcome measurement | Selective reporting/ reported Result | Other bias domains | Overall risk of bias |
|---|---|---|---|---|---|---|---|---|
| Arkkukangas et al 2022 | RoB 2.0 (RCT) | Some concerns | Some concerns | Some concerns | Some concerns | Low risk | — | Some concerns |
| Moon et al 2019 | RoB 2.0 (RCT) | Some concerns | Some concerns | Low risk | Low risk | Low risk | — | Some concerns |
| Wood et al 2019 | ROBINS-I (NRSI) | Low risk | N/A | Low risk | Low risk | Low risk | Participant selection: Low risk | Low risk |
| Del CastilloAndres et al 2018 | ROBINS-I (NRSI) | Low risk | Low risk | Low risk | Some concerns | Low risk | Participant selection: Low risk | Low risk |
| Lim and Choi 2020 | ROBINS-I (NRSI) | Low risk | N/A | Low risk | Low risk | Low risk | Participant selection: Low risk | Low risk |
| Mroczkowski 2022 | ROBINS-I (NRSI) | Low risk | N/A | Low risk | Low risk | Low risk | Participant selection: Low risk | Low risk |
NOTE: Low risk: No serious issues identified. Some concerns: Potential risk of bias in at least one domain. High risk: High likelihood of bias affecting results. N/A: Domain not applicable due to study design. RoB 2.0: Risk of Bias 2.0 tool for randomized trials ROBINS-I: Risk of Bias in Non-randomized Studies of Interventions
Discussion
This updated systematic review expands upon the work of Moons et al. by synthesizing six studies investigating the biomechanical and behavioral effects of fall landing strategies which were published after the original systematic review by Moon and Sosnoff. Of these, two were RCTs, and four were non-randomized studies. Collectively, these studies advance the evidence base regarding the feasibility, biomechanics, and potential efficacy of teaching protective fall strategies, particularly in older adult populations.
The RCTs included in this review demonstrated that older adults could learn fall landing strategies, such as the tuck-androll technique or high-challenge perturbation training, with potential improvements in confidence and reductions in impact severity [5,7]. Although both trials exhibited “some concerns” in areas such as randomization and intervention adherence, their findings support the concept that motor learning principles can be effectively applied to older adults [18].
The non-randomized studies further contextualize these findings. Three studies employed biomechanical analyses during simulated falls to examine the effect of specific landing techniques or participant characteristics on impact forces. Lim and Choi observed that tucking and rolling during backward falls reduced sagittal head acceleration, suggesting potential protective effects for head trauma prevention [17]. Similarly, Mroczkowski found that children trained in safe landing techniques significantly improved their motor responses during backward falls, providing evidence that motor learning can generalize across age groups [15]. Although this study involved a pediatric cohort, its design illustrates a model for progressive skill acquisition.
The study by Lim and Choi demonstrated that hip impact forces varied significantly based on fall characteristics such as direction, height, and anticipation [19,20]. These findings reinforce the importance of realistic fall simulation methods and further support the value of training that prepares individuals for unexpected perturbations [17]. In addition, the study by Wood et al. explored age-related differences in head impact during sideways falls. Their results revealed that older adults experienced significantly greater head acceleration compared to younger participants, underscoring the need for targeted interventions in aging populations [14].
Together, these findings converge on a few key points. First, the mechanics of fall, such as direction, initiation type, and landing position, strongly influence impact severity. Second, motor learning strategies such as tuck-and-roll or fall preparation training can be feasibly implemented in older adults. Third, while current evidence is promising, it remains limited by small sample sizes and a lack of long-term outcome data related to actual fall incidence or injury reduction.
The studies reviewed varied widely in terms of outcome measures, including impact velocity, kinetic energy, head acceleration, and qualitative skill acquisition. This heterogeneity, while reflective of the complexity and evolving nature of the field, limited the ability to pool data quantitatively through meta-analysis. Additionally, several important limitations must be considered when interpreting these findings. The overall number of eligible studies remains small, reducing the generalizability of results across broader populations. Significant variability was also present in study designs, participant demographics, fall simulation methods, and definitions of impact severity. Most studies were conducted in controlled laboratory settings, which may not fully replicate the environmental unpredictability of real-world falls. Furthermore, although some studies demonstrated short-term improvements in protective motor responses and reduced biomechanical impact, few assessed long-term skill retention or actual injury prevention. Despite these limitations, the consistent trend across studies suggests a protective benefit of safe fall landing strategies and supports the feasibility of implementing such training, particularly in older adult populations.
Conclusion
This updated systematic review supports the growing evidence that fall landing strategies can be learned and utilized by older adults to potentially reduce impact severity and injury risk. While the included RCTs offer support for intervention feasibility and short-term benefits, the biomechanical findings from non-randomized studies provide mechanistic support for the protective effects of these techniques. Future research should aim to include larger, more diverse cohorts and standardized outcome measures, and evaluate long-term effectiveness in reducing real-world fall injuries. Fall landing training may represent a valuable addition to comprehensive fall prevention programs, particularly for at-risk older adult populations.
Declarations
Conflict of interest statement: The authors declare no conflicts of interest.
The protocol was registered with the International Prospective Register of Systematic Reviews PROSPERO: #CRD42023441977.
Financial disclosure: No financial disclosures.
References
- CDC. Older adult falls data. https://www.cdc.gov/falls/data-re- search/index.html
- NCOA. Get the facts on fall prevention. https://www.ncoa.org/ article/get-the-facts-on-falls-prevention
- CDC. Patient and caregiver resources STEADI older adult fall prevention. https://www.cdc.gov/steadi/patient-resources/index. html
- Moon Y, Sosnoff JJ. Safe landing strategies during a fall: systematic review and meta-analysis. Arch Phys Med Rehabil. 2017; 98: 783-794.
- Moon Y, Bishnoi A, Sun R, Shin JC, Sosnoff JJ. Preliminary investigation of teaching older adults the tuck-and-roll strategy: can older adults learn to fall with reduced impact severity. J Biomech. 2019; 83: 291-297.
- Leonhardt R, Becker C, Groß M, Mikolaizak AS. Impact of the backward chaining method on physical and psychological outcome measures in older adults at risk of falling: a systematic review. Aging Clin Exp Res. 2020; 32.
- Arkkukangas M, Bååthe KS, Ekholm A, Tonkonogi M. High challenge exercise and learning safe landing strategies among community-dwelling older adults: a randomized controlled trial. Int J Environ Res Public Health. 2022; 19.
- Groen BE, Smulders E, De Kam D, Duysens J, Weerdesteyn V. Martial arts fall training to prevent hip fractures in the elderly. Osteoporos Int.
- Li ZR, Ma YJ, Zhuang J, et al. Ditangquan exercises based on safelanding strategies prevent falls and injury among older individuals with sarcopenia. Front Med. 2022; 9.
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA 2009 checklist. Ann Intern Med. 2014; 151.
- Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366.
- Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016; 355.
- McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012; 22.
- Wood TA, Moon Y, Sun R, Bishnoi A, Sosnoff JJ. Age-related differences in head impact during experimentally induced sideways falls. Biomed Res Int. 2019; 2019.
- Mroczkowski A. Influence of the backward fall technique on the sagittal linear acceleration of the head during a fall. Int J Environ Res Public Health. 2022; 19.
- Delcastillo-Andrés Ó, Toronjo-Hornillo L, Rodríguez-López M, Castañeda-Vázquez C, Campos-Mesa MC. Children’s improvement of a motor response during backward falls through the implementation of a safe fall program. Int J Environ Res Public Health. 2018; 15.
- Lim KT, Choi WJ. Effect of fall characteristics on the severity of hip impact during a fall on the ground from standing height. Osteoporos Int. 2020; 31.
- Ehsani F, Abdollahi I, Bandpei MAM, Zahiri N, Jaberzadeh S. Motor learning and movement performance: older versus younger adults. Basic Clin Neurosci. 2015; 6.
- Ferreira RN, Ribeiro NF, Figueiredo J, Santos CP. Provoking artificial slips and trips towards perturbation-based balance training: a narrative review. Sensors. 2022; 22.
- Bhatt T, Wang Y, Wang S, Kannan L. Perturbation training for fallrisk reduction in healthy older adults: interference and generalization to opposing novel perturbations post intervention. Front Sports Act Living. 2021; 3.